
Modeling women’s health after childbirth
Childbirth is a momentous and fraught time. For women, childbirth is one of the most significant biomechanical events in life – in terms of forces and motion, the body during childbirth is a structure stressed to extremes.
For bioengineer Steven Abramowitch, that is not a cold description. He studies damage to women’s pelvises due to pregnancy and delivery – damage that may only manifest decades after the birth. His team relies on CRC resources in modeling structures of the pelvis that indicate potential health problems.
“In the past, this aspect of women’s health has been considered ‘private’ in nature,” Abramowitch explains. “Women’s health research has always taken a backseat. Pelvic prolapse – when pelvic muscles can no longer hold up organs like the bladder – is more prevalent than conditions like ACL injuries, but no one discusses it. It’s embarrassing. It can lead to symptoms like urinary and fecal incontinence, which folks don’t like talking about.”
Abramowitch is associate professor of bioengineering at the Swanson School of Engineering and the Clinical and Translational Science Institute. His research into pelvic health disorders resulting from childbirth increasingly relies on computational models developed with CRC resources.
Computer modeling is better than studying animal models for a simple reason – animals are generally quadrupeds. Gravity does not affect their organs the same ways it affects humans. Bipedal humans inherited an evolutionary conflict between efficiently walking upright and efficiently delivering babies.
“Women’s bodies in childbirth are really at the limits of what the tissues can withstand,” Abramowitch explains. “Childbirth is associated with a lot of soft tissue injuries, many of them unrecognized because they are internal. A muscle tear or nerve damage is not obvious to the obstetrician delivering the baby.”
The injuries appear later in life, sometimes driven by a secondary event or in a degenerative process taking place over time. Modeling similarities and differences among a range of pelvic shapes, Abramowitch believes, can provide insight into the potential for injury.
Abramowitch’s team uses two methods to model pelvises – finite element analysis and statistical shape modeling of the pelvis and bones of the hip, sacrum, and coccyx, based on MRI scans.
Finite element analysis essentially breaks the complex whole of a pelvis into manageable geometric points. Collectively the discrete points create a picture of the entire system. More points create a more complete picture – and call for more computer memory and processing power.
Statistical shape modeling looks at those discrete geometric points across a population to build a statistical model of how those geometries are distributed, the goal being to analyze the same corresponding points. The geometric shapes that have been broken into small pieces are reassembled and compared – again calling for a lot of advanced computing resources.
“With the models we can say what pelvic geometries are associated with certain types of birth outcomes,” explains Abramowitch. “We can input those geometries into our models to find underlying mechanisms that might be associated with particular outcomes.”
PhD candidate Megan Routzong is part of Abramowitch’s team and lead author on a 2020 paper in the journal Computer Methods and Programs in Biomedicine – “Pelvic floor shape variations during pregnancy and after vaginal delivery.” The work used the same statistical shape modeling the team can carry out at CRC on a much bigger scale.
Routzong tells the story. “When I started this work, some family asked: ‘Why are you studying childbirth? Women have been giving birth for centuries,’ I ask, did they enjoy that experience? How many women still die from that experience or have a severe quality-of-life loss?”
“The idea behind the research is that if we define an average or typical anatomy, then the more easily a clinician would be able to identify someone whose anatomy tends toward a disease state. The question is which anatomical factors – computationally we refer to them as geometries – correlate or correspond with predicted negative vaginal birth outcomes like excessive stretching in a particular region of a muscle.”
The team creates a segmented, partial pelvis shape and a template shape and tries to fit the template shape to the segmented shape, to fill in the missing data. When a woman gets an ultrasound during pregnancy, it would be possible to use what is visible in the ultrasound field of view – which is smaller than an MRI field of view – to make predictions about how the rest of her pelvic shape might affect the delivery. The goal is reducing the amount of data need to make predictions, ultimately to create a tool that clinicians could use for every pregnancy.
Routzong works closely with graduate student Liam Martin, who performs much of the computation on Abramowitch’s team. “The team needs CRC to perform the volume of computing needed for comparisons. Even at CRC, we quickly used up most of our computing allocation. One pelvic shape alone has 100,000 points in the model. Our lab computers can’t handle that volume.”
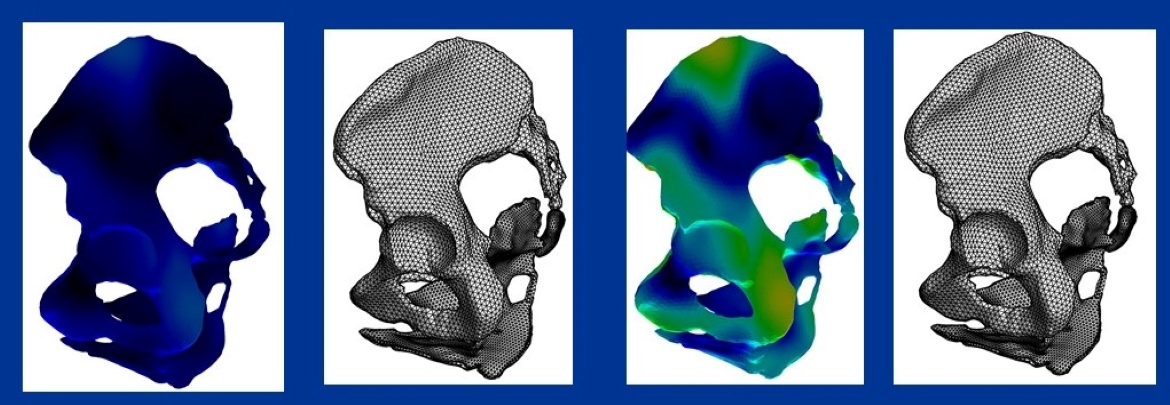
Martin explains. “The goal of the statistical shape modeling of the geometries of the pelvises is to understand more patterns of differences than could be explained by random noise. On the images of the pelvises [see the illustration above] the shapes are shaded between bright and dark colors. Closer to blue or black is the mean shape, and the brighter colors show high variability.”
“With scans of 24 pelvic geometries, we derived three average pelvises based on smoothing – an algorithm that deforms the geometries into a normal shape, average shape, and template shape. That makes it very easy to calculate an average or point-to-point comparison. Theoretically the points are in the same places and represent the same point on the same structure for every subject shape, so it allows for a lot of comparisons.”
Martin is excited about the possibilities offered by CRC. “We’re in transition from mechanical testing to computational testing, so CRC is very new for us. We’ve actively used CRC for about a year. At first it was cool to mess around with – but now CRC is implemented in our workflows.”
For Routzong, CRC was a revelation. “This kind of research would not be feasible without CRC resources. We can use CRC without already being funded, especially if you need a preliminary study before applying for the grant. A lot of the shape modeling is not possible at all on any of our machines. A colleague at another lab told me to apply to use CRC, but we didn’t have funding and I said I needed to first try every free resource. I didn’t know CRC is free.”
Abramowitch considers the potential impact of the work.
“I’m a trained bioengineer, so these problems are very interesting to me from that perspective. But they are quality of life issues. Women are deeply affected. The long-term impact of pelvic damage is not just a casual part of the aging process, like wrinkles or walking slower. These can be really catastrophic, life-altering conditions.”
Contact:
Brian Connelly
Center for Research Computing
bgc14@pitt.edu